Video Lesson

Experts you'll learn from




Written Lesson
How We Diagnose Endometriosis
Endometriosis sufferers often require multiple visits across multiple years before their condition is diagnosed. There are several reasons endometriosis is so poorly diagnosed, including:
- Endometriosis has inconsistent symptoms between patients
- Many of those symptoms are easy to mistake for symptoms of other conditions, such as irritable bowel syndrome
- General Practitioners and OBGYNs are dismissive of female patient pain and patients themselves may downplay and normalize their cramps or pain with periods
- We don’t have methods for diagnosis that are both accessible and reliable
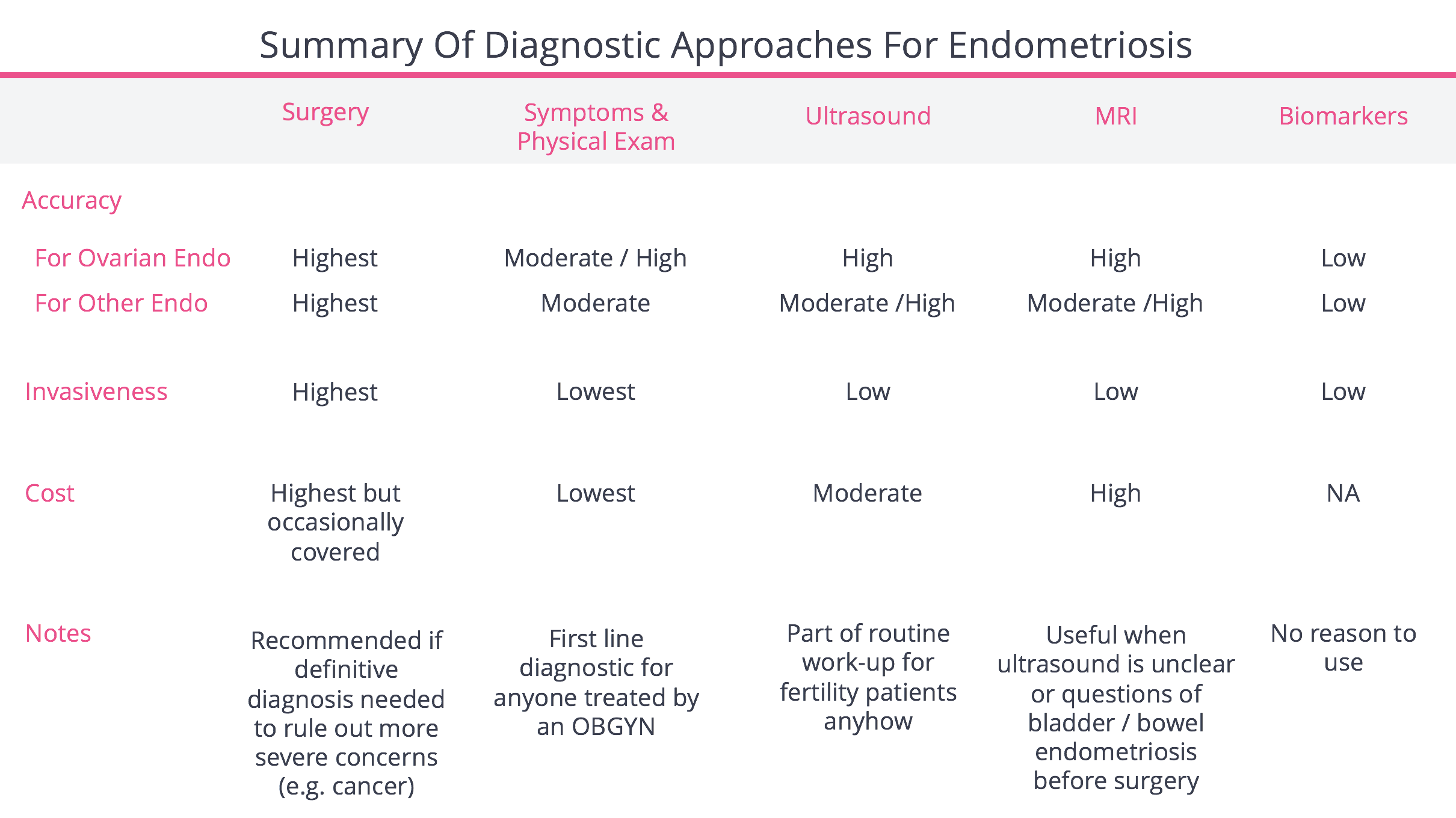
In this lesson we’ll focus on the last point, our methods for diagnosing endometriosis and the trade-offs of each, which we summarize below.
Accuracy of Tools for Diagnosing Endometriosis
Before we look at each form of diagnosis, we want to say a word about “accuracy.” Accuracy of a test can be broken down into two concepts: a test’s “positive predictive value” or PPV and its “negative predictive value” or NPV. We will refer to this constantly and so it’s worth committing to memory.
- Positive predictive value (PPV): If the test says you’re positive, you actually do have the condition. For example, if a test indicates 100 people have endometriosis but we later find out that only 99 truly have it, the test has a 99% PPV.
- Negative predictive value (NPV): If the test says you’re negative, you truly are. For example: a test says 100 patients don’t have endometriosis, but in reality 97 of those patients truly don’t have it (thus 3 patients actually do), the test as a 97% NPV.

For each of the major diagnostic modalities, we break down their level of accuracy in diagnosing endometriosis depending on where the endometriosis may reside.

Surgery as a Diagnostic
Patients can undergo surgery during which cameras or scopes are used by a gynecologist or reproductive endocrinologist to make a diagnosis of endometriosis. Surgery is the only way to definitively diagnose endometriosis and is considered “the gold standard,” but in current practice this is more a means for standardizing patients in research studies and many patients are presumably diagnosed and treated without a surgical diagnosis.

During surgery, endometriosis can be diagnosed two ways:
- Visual inspection: The surgeons sees lesions (spots of inflammation) that are consistent with endometriosis and diagnoses the patient as having it.
- Biopsy: The doctors takes biopsies, small samples of cells, that are later inspected under a microscope to see if the cells in the biopsy have endometriosis.
Surgery has a number of crucial benefits but also real drawbacks. For that reason, many doctors and societies recommend against it when used solely for the purpose of diagnosis.
Benefits of Diagnostic Surgery
Surgery as a diagnostic has five major benefits: it’s accurate, allows the doctor to treat the disease in that moment, allows the doctor to double check whether the fallopian tubes are truly open or closed, and helps the doctor characterize how widespread the disease has become.
Strong Accuracy: Surgery’s chief benefit is that it’s more accurate in diagnosing endometriosis than any other method we have. When the diagnosis is made by:
- Biopsy: The “theoretical” Positive Predictive Value (says I have it & I do) and Negative Predictive Value (says I don’t have it and I don’t) are very close to 100% because it is the most advanced tool we have for diagnosing patients. There is no more advanced test to tell us if a biopsy diagnosis is wrong.
- Visual: When a doctor says a patient has endometriosis upon visual inspection, only 50 - 80% of the cases does the patient actually have it (when compared to a biopsy that is later evaluated under the microscope.) This means visual inspection has an approximate Positive Predictive Value (says I have it & I do) of 50 - 80%, with a greater PPV in more advanced stages of endometriosis. Said differently, in 20 - 50% of cases, if a patient was diagnosed by surgical visual inspection alone as having endometriosis, the diagnosis is incorrect.
Among patients with symptoms, when the doctor does surgery and visually determines there is no endometriosis, in 6% of cases they are wrong and a biopsy reveals the patients actually do have endometriosis. This means visual inspection has a 94% Negative Predictive Value (says I don’t have it and I really don’t).

Ability To Treat At The Same Time: During diagnostic surgery, some clinicians can also treat (remove or destroy) the areas of endometriosis. As we’ll discuss in the next lesson, this has value for reducing pain, but may not necessarily improve pregnancy rates.
Ability To Inspect Fallopian Tubes: During diagnostic surgery, doctors can also inspect the fallopian tubes to determine whether they are open. Open tubes are a requirement for the sperm and egg to meet and for natural conception or intrauterine insemination (IUI), to work.
Surgical inspection is more accurate than other methods to look at the tubes like HSG or FemVue ultrasound. For instance, in 23% of cases an HSG says a woman’s tubes are closed when they are actually open. The implication is that for some patients who are told they must do IVF on account of their closed tubes, the option to conceive naturally, or through IUI, may still exist. For women who have been told they have a tubal blockage, visual inspection can be a valuable benefit of diagnostic surgery for endometriosis.

Ability To “Stage” Endometriosis: During surgery a doctor can get a sense for how widespread the endometriosis is. This often correlates into a “staging system.” The most popular staging system is the ASRM system whereby doctors rank the endometriosis on a 1 - 4 scale (4 being the most widespread).
The ASRM staging system is useful in that it can help your doctor know what research is relevant to your case and maybe the next logical step for treatment. In this regard, being able to “stage” your case is useful.
However, ASRM staging system has poor reproducibility (50% of the time doctors disagree on the stage) and has virtually no predictive value of a patient’s likelihood to conceive.
The one staging system we believe can credibly predict outcomes post-surgery is known as the Endometrial Fertility Index (EFI). We’ll address it in the next lesson where we discuss the likelihood of success by each treatment option (like surgery or IVF).
Diagnosis And Removal Of Other Abnormalities: During surgery other abnormalities can be found and can possibly be treated, namely, in very rare circumstances, ovarian cancer.
Negatives Of Diagnostic Surgery
Surgery as a diagnostic has many drawbacks and for that reason many recommend against using it purely to make a diagnosis. Here are the reasons why:
- Risk To Egg Supply: During surgical diagnosis if the doctor decides to treat (burn or cut) endometriosis on the ovary, this can impair a woman’s egg supply, reducing ovarian reserve and hurting her ability to conceive
- Risk of Complications: Roughly 1% of patients suffer issues related to the surgery or anesthesia
- Patient Inconvenience: Nearly all patients face a recovery time of 2 to 6 weeks, which can force them to miss work or the ability to handle other responsibilities
Given this, the American Society of Reproductive Medicine recommends against using surgery solely to make a diagnosis of endometriosis in patients who don’t have symptoms. However, it may be necessary if another diagnosis needs to be excluded or if your physician thinks there may be benefit of surgically treating endometriosis.
When deciding whether surgery should be used to diagnose endometriosis, you should be aware of bias from your doctor’s background. A minimally invasive surgeon or gynecologist who performs surgery frequently is more likely to recommend surgery for diagnosis. On the other hand, a reproductive endocrinologist (who belongs to ASRM, the society that recommends against surgery for diagnostic purposes) specializes in assisted reproduction and may be less likely to perform surgery and more likely to recommend other treatments like IVF. Both perspectives can be correct depending on the situation, and while potentially confusing it can often be helpful to get a second opinion before choosing a particular treatment.
Diagnosing Endometriosis Using Symptoms and Physical Exam
Because surgery is invasive, many doctors will make a “presumptive diagnosis” of endometriosis based on a patient’s symptoms. There is a long list of potential symptoms caused by endometriosis — most of which can also be caused by other conditions — making diagnosis tricky. The most common symptoms that should raise your suspicion of endometriosis include:

In conjunction with taking account of symptoms, a doctor will also perform a physical exam. During an exam, a doctor will place a duck-billed instrument called a speculum into the vagina to better visualize the cervix and vagina. Then with one hand placed on the lower abdomen and the other in the vagina, the doctor will try to palpate the uterus, ovaries, the ligaments that support the uterus, and any masses that may be present and appreciate any areas that are tender.
Occasionally, doctors will prescribe continuous birth control pills, progesterone, or lupron upon making a diagnosis based on symptoms. These drugs starve endometriosis (if it exists) of estrogen needed to grow. If the patient’s pain symptoms go away after birth control, the doctor will feel more confident in their initial presumptive endometriosis diagnosis. Of course, this will not be an option for women trying to conceive now.
Accuracy
The accuracy of taking a history and doing a physical exam is mediocre and varies depending upon where the endometriosis may reside. Accuracy for endometriosis on the ovary is higher because a doctor can barely feel a normal ovary by a physical exam. If a doctor can feel it, or it’s tender, it may well be enlarged by endometriomas (endometriosis-filled sacs on the ovary).
More problematic is that doctors doing a physical have a very low Positive Predictive Value (says I have it & I do) for endometriosis in other parts of the pelvis. In over half of the instances, when a doctors diagnoses endometriosis not on the ovary using a physical exam, the patient does not in fact have it.
While physical examination has its place, in many ways it’s inferior to a physical examination alongside ultrasound (which we’ll cover next). Since most every OBGYN has access to transvaginal ultrasound in their office, it’s often wise to insist they use it.

Clinical Correlates of Endometriosis Symptoms
Although not all women have symptoms, when there are symptoms they may correspond to specific locations where the endometriosis has spread. We’ve outlined some of the more common associations in the table below.
Diagnosing Endometriosis Using Ultrasound
During an ultrasound, a small plastic probe is placed into the vagina and repositioned until all the structures in question have been seen. It can be done in a general OBGYN provider’s office, in a radiology office, and is always performed in a reproductive endocrinologists office as part of an infertility workup. Ultrasound is the imaging study of choice in diagnosing endometriosis according to American College of Obstetrics and Gynecology. Its major drawback deals in issues of accuracy when diagnosing non-ovarian endometriosis.

Accuracy
Generally speaking, the accuracy of ultrasound for diagnosing endometriosis is solid (better than a physical exam, worse than surgery). As for detecting endometriosis on the ovary, ultrasound is a good tool, as you can see below. For that reason, ultrasound has a good Positive Predictive Value (says I have it & I do) and Negative Predictive Value (says I don’t have it & I don’t).

However, ultrasound is far less reliable in diagnosing endometriosis elsewhere in the pelvis. Specifically, the Positive Predictive Value (says I have it & I do) is as low as 50%, leading many women to being wrongly told they have endometriosis, when they don’t. You’ll recall physical exams suffer from this exact same issue — in this regard ultrasound is likely better, though still not good.

Using MRI to Diagnose Endometriosis
Like ultrasound, Magnetic Resonance Imaging (MRI) is an imaging technique that takes pictures of internal structures. During an MRI, patients are asked to lie still on a bed that slides slowly through a machine. A doctor who specializes in medical imaging, a radiologist, looks at the images and makes a determination if there is endometriosis.
Generally speaking, MRI is no better than ultrasound, but is far less accessible and more costly, so it’s often a worse option. That said, MRI is invaluable in diagnosing endometriosis on the bowel or bladder and, when there is a credible reason it could reside there, MRI can have a valuable role to play in diagnosing it and planning for surgery.

One final word to say about MRI is that the accuracy data we display here is probably the best one could expect from MRI. Ours comes from studies using expert radiologists to interpret the images. Many radiologists are generalists and likely few are as competent as those participating in studies. MRI’s accuracy, in less experienced hands, may be quite a bit worse.

The usefulness of MRI as a diagnostic modality is only as good as the quality of the pre-protocols in place, the quality of the images captured, and the expertise of the radiologist who is reading the images. Below are the consensus guidelines derived from the European Society of Urogenital Radiology (ESUR) that should be followed when using MRI to diagnose endometriosis. We suggest talking with your doctor and clinic about why they’re necessary and whether your clinic is prepared to incorporate. Also, ideally, the radiologist reading the images will have GYN-specific training and you should feel free to ask your doctor if the institution has a specialized radiologist who is experienced with diagnosing endometriosis via MRI.
Guidelines when using MRI to diagnose endometriosis:
- Patients should fast for 3-6 hours before the appointment to reduce peristalsis artifacts. Another option is the administration of intravenous or intramuscular glucagon as an anti-peristaltic agent.
- Patients should abstain from urinating 1 hour before the appointment because bladder distention helps identify bladder lesions.
- T2W imaging in at least 3 planes and T1W with and without fat suppression is recommended.
- Post contrast imaging with IV gadolinium.
- Use of structured radiologic reports tailored to the evaluation of endometriosis. These provide an organized framework of the pertinent data in an effort to provide comprehensive patient counseling and treatment planning.
Biomarkers for Diagnosing Endometriosis
Biomarkers are an attractive diagnostic method for any medical condition, in theory providing a diagnosis with a simple blood test. For example, hCG is produced by a pregnancy and when it’s present in the blood, accurately reflects a pregnancy is underway. Unfortunately no biomarker is currently accurate enough to be recommended to diagnose endometriosis.
CA-125, a biomarker used to follow certain ovarian cancers, is often elevated in patients with endometriosis. While a recent meta-analysis demonstrated specificity (when the test says you have it, you actually have it) of 93%, its ability to detect all women who have endometriosis (known as sensitivity) is low (52%) and even lower for patients with mild or moderate endometriosis. Research is underway to develop more accurate biomarkers for endometriosis so hopefully a blood test, rather than a surgery, will be all that is required for a definitive diagnosis in the future.
An additional biomarker, BCL6, has been shown to be correlated in patients with endometriosis. Investigators have evaluated BCL6 for use as a non-invasive indicator of endometriosis, however, at this time, it can still only be tested by means of an endometrial biopsy, which is significantly more invasive than a simple blood test.
BCL6 testing is now being offered to some patients under the brand name ReceptivaDX.
We discuss treatment options for patients testing positive for BCL6 in the next lesson.
Pro Tips
- There is often to a delay in diagnosis of up to a decade for many patients
- Painful periods, pain with sex, non-cyclical pelvic pain, infertility and fatigue are warning signs you may have endometriosis. If you have these symptoms and your doctor does not bring up the possibility of endometriosis first, you should bring it up and discuss additional diagnostic methods
- Surgery is the only way to definitively diagnose endometriosis. Biopsy is more accurate than visual inspection
- Surgery is invasive and should not be used purely for diagnostic purposes other than to rule out more serious concerns (like cancer)
- For non-surgical means of detection, generally speaking, doctors more accurately diagnose endometriosis on the ovaries than in other parts of the pelvis
- Physical exams are easy for many doctors to perform and have generally good accuracy, especially when it comes to ruling in, or out, endometriosis on the ovary
- However, when doctors declare, after physical exam, a patient has endometriosis elsewhere in the pelvis, they are wrong about half of the time. This results in patients being diagnosed with endometriosis who don’t have it
- Ultrasounds are provided for every patient that goes to a fertility clinic. They are relatively inexpensive, non-invasive and easy to read. They are the default diagnostic for identifying if an infertile patient has endometriosis
- Ultrasound is good at ruling in, or out, endometriosis on the ovary. However, it can be less accurate for diagnosing endometriosis in other parts of the pelvis
- MRI is usually not necessary for diagnosis, but it should be considered for patients exhibiting signs of bowel or urinary pain as MRI is good at detecting endometriosis on these organs and it can be helpful for planning surgery in these areas
- Endometriosis surgery, if necessary, is more complicated if it involves the bowel or intestines. An MRI is useful in helping to plan surgery in these cases
- CT scans, X-rays, and other imaging are usually not helpful, and expose patients to unneeded radiation
- Unfortunately there is no blood test for endometriosis that’s ready for prime time